What are other Names for this Condition? (Also known as/Synonyms)
- Leiomyosarcoma of Uterine Corpus
- Leiomyosarcoma of Uterus
- ULMS (Uterine Leiomyosarcoma)
What is Uterine Leiomyosarcoma? (Definition/Background Information)
- Leiomyosarcoma (LMS) is a rare type of connective tissue cancer, accounting for 5-10% of all soft tissue sarcomas, which are a type of cancer. Experimental analysis point to the cell line origin for leiomyosarcoma being smooth muscle cells
- Uterine Leiomyosarcoma or Leiomyosarcoma of Uterine Corpus is the most frequent subtype of uterine sarcoma in women. They are known to originate from the muscular wall of the uterus known as the myometrium
- The cancer generally affects women after menopause (age 50 years and above). Women, who are on tamoxifen treatment for breast cancer, have a very high risk for Uterine Leiomyosarcoma. The cause of the cancer is related to genetic factors and chromosomal aberrations
- The signs and symptoms of Uterine Leiomyosarcoma include unusual vaginal bleeding, discharges, and sensation of pressure in the pelvic area. The complications are dependent upon the stage of the cancer and the method of treatment employed. Advanced stage tumors are observed to metastasize to the lungs
- Treatment for the malignancy is mainly through surgery and supplementary treatment measures that include radiation therapy and chemotherapy. The prognosis of Uterine Leiomyosarcoma mostly depends on the cancer stage and other factors. However, the prognosis of the condition is generally poor
There are several morphological variants of Leiomyosarcoma of Uterine Corpus. The variants include:
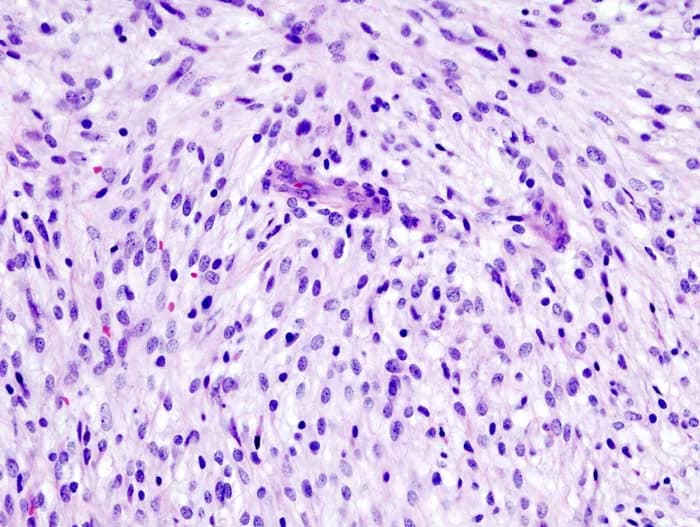
- Spindle Cell Leiomyosarcoma
- Epithelioid Leiomyosarcoma
- Myxoid Leiomyosarcoma
Who gets Uterine Leiomyosarcoma? (Age and Sex Distribution)
- Leiomyosarcoma is the most common sarcoma affecting the uterus. It constitutes 1-2% of all cancers of the uterus
- Nevertheless, Uterine Leiomyosarcoma is a rare form of cancer; only 3-4 women per million women may be affected worldwide
- Middle-aged and older adults are generally affected by LMS, even though a wide age range may be observed. Typically, women between the ages of 40 and 60 years are most susceptible to Uterine Leiomyosarcomas. Most cases are seen in women over 50 years of age
- There are no known geographical localizations and this cancer type is found worldwide among all races and ethnic groups
What are the Risk Factors for Uterine Leiomyosarcoma? (Predisposing Factors)
While there are no clearly-established risk factors for Uterine Leiomyosarcomas, there are a few leading theories:
- Use of the drug tamoxifen for treatment of breast cancer: The incidence of Uterine Leiomyosarcoma in women with therapy using tamoxifen for breast cancer is much higher than that observed among the general population
- Certain inherited genetic traits are believed to increase the risk, even though this factor has not been adequately substantiated
- High-dose radiation exposure to the uterine region, such as pelvic radiation therapy, is believed to increase the risk for leiomyosarcoma
- Being born with an abnormal copy of the RB (retinoblastoma) gene may increase one’s risk. Retinoblastoma, a type of eye cancer, may also arise from an abnormal copy of this gene
- Immunocompromised patients infected by Epstein-Barr virus seem to be predisposed to LMS. The reason for this is not understood, yet there seems to be a definite correlation between the viral infection and the arising of multiple, synchronized leiomyosarcomas
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases ones chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Uterine Leiomyosarcoma? (Etiology)
Currently, the exact cause of Uterine Leiomyosarcoma, a smooth muscle malignancy, is not clearly identified or evident. Smooth muscles are muscles that are not voluntarily controlled. Due to the bounty of smooth muscle throughout the body, any individual is susceptible to LMS. However, due to the rarity of the cancer, it is difficult to determine what exactly leads to the formation of Leiomyosarcoma of Uterine Corpus.
- In general smooth muscle tumors, such as leiomyosarcomas, are known to have genomic instability. Chromosomal aberrations (loss or gain of chromosomal pieces) have also been noted in the tumors
- Overexpression of the proto-oncogene c-MYC is noted in 50% of the tumors; retinoblastoma gene associated discrepancies are seen in 90% of the tumors
- Some studies have revealed p-16 chromosomal deletion causing loss of tumor suppression in the tumors
- Uterine Leiomyosarcoma is thought to occur spontaneously due to genetic anomalies; a family history is not known to be present, unlike leiomyomas
- Also, the possibility of a malignant transformation of leiomyomas to leiomyosarcomas is under research. Presently, it has not been conclusively proven that such malignant transformations can take place
What are the Signs and Symptoms of Uterine Leiomyosarcoma?
The following features of Uterine Leiomyosarcoma (ULMS) may be generally observed in women:
- Many LMS of Uterus are solitary in nature, but they can be also seen in association with benign leiomyomas. When in association with leiomyomas, the cancer can grow to very large sizes
- Many signs and symptoms of LMS of Uterus overlap with those of uterine leiomyomas (which are commonly known as uterine fibroids)
- Most tumors are about 10 cm on detection; it is uncommon to find tumors below 5 cm in size (which, studies have shown, is noted only in 1 in 4 cases)
- The tumors appear as a soft and firm mass with irregularly-defined boundaries
- The tumors may be classified according to the location, and may be:
- Intramural tumors, found within the uterine walls; 65% of the tumors are of this type
- Submucosal tumors, found in the thin tissues beneath the mucosal layers; 20% of the tumors are of this type
- Subserosal tumors, found in the connective tissues (beneath the serosal layers); 10% of the tumors are observed on the serosa
- Generally, 5% of the remaining leiomyosarcomas are seen in the uterine cervix
- Tumors at submucosal and subserosal locations are usually like a polyp, or hang in a bag-like structure (known as pedunculated tumors)
The signs and symptoms of Uterine Leiomyosarcoma may include the following:
- Vaginal bleeding and the presence of a mass that may be felt in the pelvic region are seen in 50% of the cases
- Pain in the pelvis is noted in about 25% of the cases; some tumors are very painful
- Unusual feeling of fullness in the pelvic region: In some cases, a swollen mass that bulges out of the uterus is noted; as much as 50% of the tumor mass can be out of the uterus
- Vaginal discharge
- Enlargement of lower abdomen; abdominal pain
- Frequent urination due to compression/pressure of the tumor
- Lower back pain
- Pain during sexual intercourse
- Bleeding can occur within large tumors (hemorrhage)
- Hemorrhage within the tumors can lead to tissue death (infarction)
Less frequent signs and symptoms of ULMS include:
- Weight loss
- Weakness and lethargy
- Fever
- In few cases, rupture of tumor and bleeding may be the first indications of the malignant tumor. This results in retroperitoneal bleeding
It is important to note that there are no specific clinical features that can be used to discern leiomyosarcoma from other soft tissue sarcomas of the uterus. Biopsies are often necessary to determine if a Uterine Leiomyosarcoma is present.
How is Uterine Leiomyosarcoma Diagnosed?
A diagnosis of Uterine Leiomyosarcoma may be made by using the following resources:
- Preliminary examination composed of:
- Complete physical examination
- Evaluation of medical (and family) history
- Initial diagnosis that is made by:
- Transvaginal ultrasound of the uterus can provide an image of the uterus and surrounding pelvic organs, along with determination of the presence of a tumor affecting the myometrium of the uterus
- MRI scans can be used to observe if a uterine tumor has the characteristics of cancer, along with visualizing the cancer spread (if it has spread to other areas)
- Plain radiographs of the chest can provide evidence if the tumor has spread to the lungs
- CT scans are rarely used in diagnosing uterine cancer, but can be used to determine if metastasis has occurred
- Blood tests that include:
- Complete blood count (CBC) to detect the cause of anemia
- Determination of estrogen/progesterone levels in blood
- A hysteroscopy may be performed to visualize and simultaneously perform the biopsy of any abnormal growth within the uterus. A hysteroscopy is performed with the aid of a tiny telescope through the uterus that allows a visualization of the area
- Hysterosalpingography: It is usually performed in individuals with infertility. In this procedure, the structure of the uterus and fallopian tubes are studied by using a dye and X-ray images
- Needle biopsy of tumor: A needle biopsy may not be helpful, because one may not be able to visualize the different morphological areas of the tumor. Hence, a needle biopsy as a diagnostic tool has certain limitations, and an open surgical biopsy is preferred
- Open biopsy of tumor: A tissue biopsy is performed and sent to a laboratory for a pathological examination, who examines the biopsy under a microscope. After putting together clinical findings, special studies on tissues (if needed) and with microscope findings, the pathologist arrives at a definitive diagnosis
- Differential diagnosis, to eliminate other tumor types is considered, before arriving at a definitive diagnosis of Leiomyosarcoma of Uterus
Note: Many features of a Uterine Leiomyosarcoma are similar to those of a benign uterine leiomyoma. In such cases, if the signs and symptoms of a leiomyoma are noted in a woman younger than 45 years, who is not undergoing any hormonal therapy, Uterine Leiomyosarcoma should be strongly suspected.
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are possible Complications of Uterine Leiomyosarcoma?
The possible complications of Uterine Leiomyosarcoma include:
- Stress and anxiety due to cancer of the uterus
- Heavy and prolonged menstrual bleeding may result in anemia
- Polypoid tumors may undergo mechanical injury, such as torsion or twisting, which can result in excruciating pain. Polyp-shaped tumors are known to cause cervical prolapse in some cases
- Some tumors grow to large sizes and even grow out of the uterus, affecting the adjoining reproductive organs
- The cancer can spread in any direction, even regionally; they can cause gastrointestinal tract or urinary tract signs and symptoms
- The rarity of the condition may cause a delayed diagnosis, leading to metastasis
- Metastasis is likely to occur in the early stages of Uterine Leiomyosarcoma, due to the high vascularity (blood supply) of the uterus. Typically, metastasis from ULMS initially appears in the lungs
- The tumor may also adversely impact adjoining/surrounding structures, such as the nerves and joints, leading to discomfort or a loss of feeling
- Side effects of chemotherapy (such as toxicity) and radiation
- Sexual dysfunction can take place as a side effect of surgery, chemotherapy, or radiation therapy
- Recurrence of the cancer following incomplete surgical removal
How is Uterine Leiomyosarcoma Treated?
Once a diagnosis of cancer of the uterus has been made, the extent to which the tumor has spread is assessed. This is called staging.
Following is the staging protocol for uterine cancer, according to the American Joint Committee on Cancer (AJCC), updated July 2016:
Stage I uterine cancer: The cancer is found in the uterus only. Stage I is divided into stages IA and IB, based on how far the cancer has spread.
- Stage IA: The cancer is in the endometrium only or less than halfway through the myometrium (muscle layer of the uterus).
- Stage IB: The cancer has spread halfway or more into the myometrium.
Stage II uterine cancer: The cancer has spread into connective tissue of the cervix, but has not spread outside the uterus.
Stage III uterine cancer: The cancer has spread beyond the uterus and cervix, but has not spread beyond the pelvis. Stage III is divided into stages IIIA, IIIB, and IIIC, based on how far the cancer has spread within the pelvis.
- Stage IIIA: The cancer has spread to the outer layer of the uterus and/or to the fallopian tubes, ovaries, and ligaments of the uterus.
- Stage IIIB: The cancer has spread to the vagina and/or to the parametrium (connective tissue and fat around the uterus).
- Stage IIIC: The cancer has spread to lymph nodes in the pelvis and/or around the aorta (largest artery in the body, which carries blood away from the heart).
Stage IV uterine cancer: The cancer has spread beyond the pelvis. Stage IV is divided into stages IVA and IVB, based on how far the cancer has spread.
- Stage IVA: The cancer has spread to the bladder and/or bowel wall.
- Stage IVB: The cancer has spread to other parts of the body beyond the pelvis, including the abdomen and/or lymph nodes in the groin.
(Source: Stages of Uterine Cancer, July 2016, provided by the National Cancer Institute at the National Institutes of Health; U.S. Department of Health and Human Services)
In general, Leiomyosarcoma of Uterine Corpus is a highly-aggressive cancer and the treatment can be challenging. A multidisciplinary approach with a team of healthcare specialists and experts from various medical fields may be necessary to treat the cancer at a healthcare institution that has the experience and expertise in dealing with such high-grade cancers.
Surgery is the most common treatment for Uterine Leiomyosarcomas.
- Hysterectomy: A hysterectomy, or removal of the uterus, is the most common treatment procedure for localized (non-metastasized) cancer. In this procedure, the uterus and cervix are removed. This is done by making an incision on the abdomen (termed abdominal hysterectomy), or through the vagina (termed vaginal hysterectomy), or by using a laparoscope (termed laparoscopic hysterectomy). Surgery is performed under general or epidural anesthesia, though the ability to have children is lost. Complications, such as bleeding, infection, or damage to the urinary tract, or the intestinal system may occur in rare cases
- Radical hysterectomy: A radical hysterectomy, removal of the uterus and tissues surrounding it, may be performed. But, this is typically more suited for tumors that have spread beyond the uterus. The uterus, cervix, the upper part of the vagina and tissues, next to the uterus are removed. Additionally, some pelvic lymph nodes may also be surgically taken out. The surgery is performed under anesthesia and may be carried out, via an incision made on the abdomen or by using laparoscopy. With this invasive procedure, the ability to have children is lost. Rarely, complications such as bleeding, infection, or damage to the urinary tract or the intestinal system, may occur. Removal of lymph nodes may lead to swelling of legs (lymphedema)
- Pelvic exenteration: The uterus, tissues surrounding the uterus, cervix, pelvic lymph nodes, and the upper part of the vagina, are removed. In addition, depending on the tumor spread, the remainder of the vagina, the bladder, rectum, and a part of the colon, may also be removed. Recovery from this surgery takes a long period
- Although Leiomyosarcoma of the Uterus has the ability to spread to the surrounding lymph nodes, a lymph node resection has not yet proven to be therapeutic
- Arterial embolization may be used to provide temporary relief from the symptoms, and reduce blood loss during a surgical procedure
- Post-operative care is important: One must maintain minimum activity levels, until the surgical wound heals
Chemotherapy:
- Medications are used to kill the tumor cells, which may be given as oral pills or injected into veins
- A combination of chemotherapy medications may be used
Radiation therapy:
- This procedure uses high-energy beams to kill the cancer cells
- These beams may be delivered from outside the body (external beam radiation therapy) or the radioactive material maybe placed inside the vagina or the uterus (internal radiation therapy or brachytherapy)
Other than surgery, LMS provides a treatment challenge due to the observed resistance to chemotherapy and radiation therapy.
In addition to traditional adjuvant therapies, the following techniques are currently being investigated:
- Immunotherapy aims to stimulate the patient’s immune system to recognize and destroy the cancer cells. It includes:
- Antigen vaccines
- DNA vaccines
- Viral therapy
- Gene therapy
- Currently, clinical trials on adjuvant chemotherapy and combinational chemotherapy, as secondary treatment to hysterectomy, are showing promising results on reducing the risk of relapse
Many patients with metastatic or locally advanced tumors may be referred for clinical trials for experimental treatment options.
Once treatment is complete, it is recommended that the patient schedule regular check-ups (and for a long duration of time), based on the recommendation of the specialist treating them.
How can Uterine Leiomyosarcoma be Prevented?
- There are currently no known methods of preventing Uterine Leiomyosarcoma (Leiomyosarcoma of Uterine Corpus)
- Due to its high metastasizing potential and recurrence rate, regular medical screening at periodic intervals with blood tests, scans, and physical examinations, are mandatory for those who have already been treated for this tumor
What is the Prognosis of Uterine Leiomyosarcoma? (Outcomes/Resolutions)
- Typically, the prognosis of Uterine Leiomyosarcoma is poor, even if the tumor is localized or contained within the uterine corpus. The overall 5 year survival rate is between 15-25%; for stage I & II, it is 40-70%. The stage of the tumor is the strongest prognostic indicator
- In case the tumor is contained within the uterus, then the tumor size is the most significant prognostic factor; a tumor size of 5 cm or lower has a better prognosis and consequently better survival rate
- Some studies inform that cell division activity can also dictate tumor progression and outcomes. Also, in a few studies, premenopausal women seem to fare better than postmenopausal women, when all the other factors were considered equal
- The prognosis for Leiomyosarcoma of Uterus depends upon a set of several factors that include:
- The size of the tumor and the extent of its invasion: Individuals with small-sized tumors fare better than those with large-sized tumors
- Stage of cancer: With lower-stage tumors, when the tumor is confined to site of origin, the prognosis is usually excellent with appropriate therapy. In higher-stage tumors, such as tumors with metastasis, the prognosis is poor
- Cell growth rate of the cancer (its ki-67 value): The ki-67 value is based on a protein found in cells that is a good indicator of how fast the tumor cells are growing. The ki-67 value is determined by a pathologist and is usually mentioned in the pathology report. Generally, much higher Ki-67 levels are seen in leiomyosarcomas than leiomyomas
- Overall health of the individual: Individuals with overall excellent health have better prognosis compared with those with poor health
- Age of the individual: Older individuals generally have poorer prognosis than younger individuals
- Individuals with bulky disease have a poorer prognosis
- Involvement of the regional lymph nodes, which can adversely affect the prognosis
- Involvement of vital organs may complicate the condition
- The surgical respectability of the tumor (meaning, if the tumor can be removed completely)
- Whether the tumor is occurring for the first time, or is a recurrent tumor. Recurring tumors have worse prognosis compared to tumors that do not recur
- Response to treatment: Tumors that respond to treatment have better prognosis compared to tumors that do not respond to treatment
- Progression of the condition makes the outcome worse
- An early diagnosis and prompt treatment of the tumor generally yields better outcomes than a late diagnosis and delayed treatment
- The combination chemotherapy drugs used, may have some severe side effects (like cardio-toxicity). This chiefly impacts the elderly adults, or those who are already affected by other medical conditions. Individuals, who tolerate chemotherapy sessions better, generally have better outcomes
- While removal of the uterus is the most commonly practiced treatment, recurrence of leiomyosarcoma may occur, especially in the pelvic area. The spindle cell variant of Uterine Leiomyosarcoma is known to recur early (usually within 2 years), while the epithelioid and myxoid variants may not recur for a long time (may take up to 10 years)
- Thus, it is very important to schedule and attend follow-up appointments with the healthcare provider, sometimes for several years or decades
Additional and Relevant Useful Information for Uterine Leiomyosarcoma:
- Removal of the uterus will cause the regular menstrual bleeding to stop. This also means that a woman may not have children after uterus removal; though, sexual intercourse is still possible
- Although leiomyosarcomas are rare cancer forms, there are many online discussion groups, local groups, and sarcoma centers available to provide help and support
- Based on data from the United States, Uterine Leiomyosarcomas are twice as common in African-American women as in other races

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.