What are the other Names for this Condition? (Also known as/Synonyms)
- Superficial Basal-Cell Cancer of Skin
- Superficial BCC of Skin
What is Superficial Basal Cell Carcinoma of Skin? (Definition/Background Information)
- Basal cell carcinoma (BCC) of skin is a malignant cancer affecting the skin. It is a slow-growing tumor generally observed in older individuals, in both men and women. This malignant carcinoma, which may be present as a lesion on the sun-exposed areas of the body, has an extremely rare potential to metastasize (spread) to the lymph nodes or internal organs
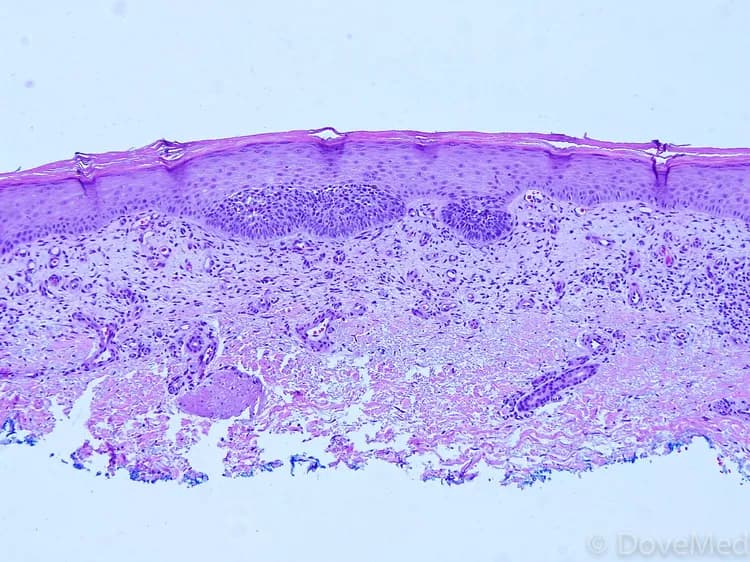
- Superficial Basal Cell Carcinoma of Skin is one of the most common types of BCC that is usually present as an erythematous (red) patch on skin of the chest and back. By definition, Superficial Basal Cell Carcinoma of Skin only involves the base of the epidermis, the outermost layer of skin. When treated early, the deeper layers of skin are not involved and do not have to be damaged by treatment
- Another feature of Superficial Basal Cell Carcinoma is their possibility to be more extensive than the clinical picture would suggest. There are also sometimes areas of normal skin, not involved with the carcinoma between carcinoma fields. If these ‘skip areas’ are not detected and treated, the carcinoma Is likely to not be effectively treated
- The cause of Superficial Basal Cell Carcinoma of Skin is unknown, but factors such as chronic sun exposure, smoking, and ionizing radiation, are known to contribute towards its development. Also, fair-skinned Caucasians have a greater risk for developing the condition than dark-skinned Africans and Asians
- Some lesions may grow to large size. If neglected, they might become invasive. Larger lesions also have a greater tendency to recur after treatment. Superficial Basal Cell Carcinoma of Skin can be treated by a variety of means, including topical creams and surgical procedures that can be curative
Who gets Superficial Basal Cell Carcinoma of Skin? (Age and Sex Distribution)
- Superficial Basal Cell Carcinoma of Skin generally affects elderly (older) adults; some cases rarely develop in children and young adults too
- Superficial BCC of Skin constitutes approximately 15% of all Basal Cell Carcinoma of Skin types. It is the second most common type of BCC of Skin
- It can occur in both males and females; however;
- Among the older age group, males are affected more than females
- In the younger age group, females are affected more than males, which may be attributed to their tendency to acquire sun-tanned bodies or visit skin tanning parlors more
- This condition is observed worldwide across all racial and ethnic groups; however, lighter-skinned individuals (especially Caucasians) are more prone to Superficial BCC of Skin than darker-skinned individuals (such as Asians, Africans, etc.)
What are the Risk Factors for Superficial Basal Cell Carcinoma of Skin? (Predisposing Factors)
The risk factors that contribute to Superficial Basal Cell Carcinoma of Skin formation include:
- Prolonged sun exposure, exposure to ultraviolet (UV) light
- Use of tanning beds, tanning parlors
- Arsenic exposure
- Ionizing radiation
- Smoking
- The presence of certain genetic syndromes such as basal cell nevus syndrome (a rare autosomal dominant disorder) increases the risk
- Caucasians are more vulnerable compared to other darker-toned individuals
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases one's chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Superficial Basal Cell Carcinoma of Skin? (Etiology)
- The exact cause of development of Superficial Basal Cell Carcinoma of Skin is not completely known, in a majority of cases
- Although, genetic mutations have been detected in Basal Cell Carcinomas, which are currently being characterized
- Most BCCs are sporadic in origin i.e., they occur in a random fashion
What are the Signs and Symptoms of Superficial Basal Cell Carcinoma of Skin?
Superficial Basal Cell Carcinoma of Skin signs and symptoms may include:
- Superficial BCC of Skin is a slow-growing malignant tumor. The tumor has a typical presentation with a flat, pink, well defined patch, usually without scale
- The surface of the patch appears red (erythema), when intact. Else, it may appear with small erosions, if the surface has been traumatized
- The patches are often many in numbers and are typically observed on the chest and back (trunk), and other sun-exposed areas
- In children, if it is associated with basal cell nevus syndrome, then multiple lesions may be observed
- The lesions may range in size from a few millimeters to up to 10 cm
- The lesion may grow and there may be itching sensation, ulceration, and bleeding
How is Superficial Basal Cell Carcinoma of Skin Diagnosed?
Some of the tests that may help in diagnosing Superficial Basal Cell Carcinoma of Skin include:
- Complete physical examination with detailed medical history evaluation
- Examination by a dermatologist using a dermoscopy, a special device to examine the skin
- Wood’s lamp examination: In this procedure, the healthcare provider examines the skin using ultraviolet light. It is performed to examine the change in skin pigmentation
- Skin or tissue biopsy: A skin or tissue biopsy is performed and sent to a laboratory for a pathological examination, who examines the biopsy under a microscope. After putting together clinical findings, special studies on tissues (if needed) and with microscope findings, the pathologist arrives at a definitive diagnosis
- Differential diagnosis of other tumors should be ruled out; hence, a skin tissue biopsy is an important diagnostic tool
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of Superficial Basal Cell Carcinoma of Skin?
The complications of Superficial Basal Cell Carcinoma of Skin could include:
- If the tumor becomes big, or ulcerates, it can get secondarily infected with bacteria or fungus
- If left untreated, Superficial Basal Cell Carcinomas can become invasive
- Superficial BCC of Skin can cause cosmetic issues
- Recurrence of the tumor after a period of time; recurrences are frequently noted with large tumors
- Effects of surgical or topical treatments, which involve scarring, redness, or secondary infection
How is Superficial Basal Cell Carcinoma of Skin Treated?
In general, the treatment of Superficial Basal Cell Carcinoma of Skin depends upon a variety of factors including:
- The location of the tumor
- The number of tumors
- The size of the tumor
- Any health considerations of the patient
A number of treatment methods may be used to treat Superficial Basal Cell Carcinoma of Skin. The treatment types may include:
Topical medications can be used to treat Superficial Basal Cell Carcinoma. This is because the thinness of the tumor permits permeation of the active ingredient to the full depth of the carcinoma. The two most frequently used active ingredients are imiquimod and 5-Flurouracil.
- Imiquimod is an immune system signal which calls for the migration of T-cells into the area of the tumor, which actively kill the cancer cells
- 5-Flurouracil is a metabolic agent which toxically kills the more basal cell carcinoma cells. The surrounding normal skin does not absorb the medication and hence is safe from the toxicity
Both these topical applications take at least a few weeks to treat a typically sized lesion, longer for larger lesions. The actions will lead to redness, irritation, sometimes crusting and possibly secondary infection
One advantage of these creams is that it is sometimes possible to treat the Superficial Basal Cell Carcinoma without affecting the underlying skin at all, so after healing, little to no scarring is detectable.
- Curettage and cautery: This is a readily performed procedure
- Mohs surgery: In this procedure, the tumor is removed layer by layer precisely, until clear margins are achieved. Each layer removed is examined under a microscope through a ‘frozen section’ procedure for the presence of residual tumor
Other techniques to treat this skin cancer (sometimes, when surgery may not be an option) may include:
- Photodynamic therapy: In this procedure, a chemical cream is applied onto the tumor, which sensitizes the tumor to light (photosensitization). After the cream application, the tumor is exposed to light. This combination of chemical therapy and light therapy kills the tumor. Usually this technique results in good cosmetic outcomes. This would be an off-label treatment under FDA guidelines
- Cryotherapy: Here the tumor tissue is destroyed through a freezing technique. Typically, liquid nitrogen is used to freeze the tumor
Note: If multiple lesions occur in children, then the possibility of basal cell nevus syndrome should be eliminated.
Generally, proper follow-up care with regular screening and check-ups are important and encouraged. In the case of large lesions, close follow-up and periodic observation is essential, since they have a tendency to recur.
How can Superficial Basal Cell Carcinoma of Skin be Prevented?
Currently, Superficial Basal Cell Carcinoma of Skin is a malignant skin cancer that has no preventive measures. However, the following factors may help reduce the risk for the condition:
- Avoid or minimize sun exposure
- Limit the use of tanning beds and tanning parlors
- Smoking cessation
- If it is caused by certain underlying disorders, then treating the underlying disorder may help in the treatment and early cure of BCC of skin
Regular medical screening at periodic intervals with blood tests, scans, and physical examinations, are mandatory, due to its metastasizing potential and high possibility of recurrence. Often several years of active vigilance is necessary
What is the Prognosis of Superficial Basal Cell Carcinoma of Skin? (Outcomes/Resolutions)
- In general, the prognosis of Superficial Basal Cell Carcinoma of Skin is excellent, if it is detected and treated early.
- Stage of tumor: With this lower-stage tumor, the prognosis is usually excellent with appropriate therapy
- The surgical resectability of the tumor (meaning if the tumor can be removed completely)
- Overall health of the individual: Individuals with overall excellent health have better prognosis compared to those with poor health
- Age of the individual: Older individuals generally have poorer prognosis than younger individuals
- Whether the tumor is occurring for the first time, or is a recurrent tumor. Recurring tumors have a poorer prognosis compared to tumors that do not recur
- Without treatment (or with delayed treatment), Superficial Basal-Cell Cancer of Skin can become invasive. This may result in a poor prognosis
- Close and regular follow-up and long-term monitor for recurrence of BCC has to be maintained
Additional and Relevant Useful Information for Superficial Basal Cell Carcinoma of Skin:
There are multiple types of Basal Cell Carcinoma of Skin:
- Superficial Basal Cell Carcinoma of Skin
- Nodular Basal Cell Carcinoma of Skin
- Infiltrating Basal Cell Carcinoma of Skin
- Micronodular Basal Cell Carcinoma of Skin
- Fibroepithelial Basal Cell Carcinoma of Skin
- Basal Cell Carcinoma of Skin with Adnexal Differentiation
- Basosquamous Carcinoma of Skin
- Keratotic Basal Cell Carcinoma of Skin

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.