What are the other Names for this Condition? (Also known as/Synonyms)
- Stage III Melanoma
- Stage IV Melanoma
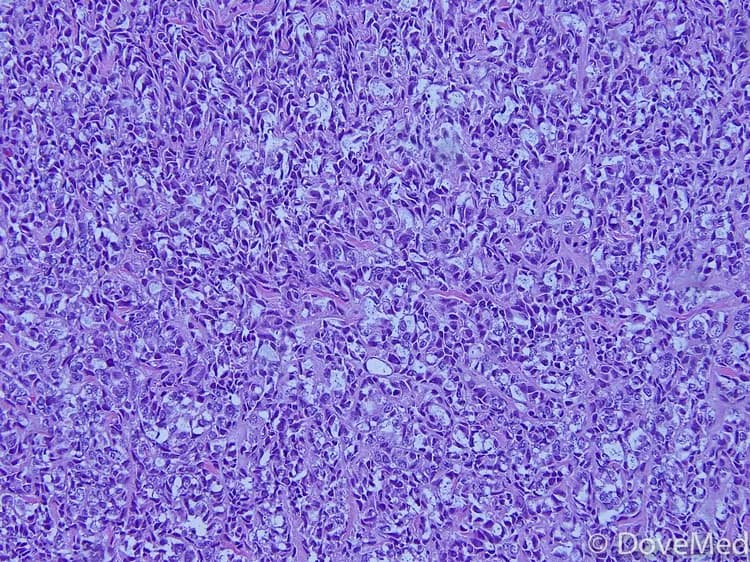
What is Metastatic Melanoma? (Definition/Background Information)
- A melanoma is a type of cancer that develops from cells, called melanocytes. Melanocytes are cells that produce melanin; the pigment that gives skin its color
- Although a less common form of skin cancer, it is far more dangerous and capable of spreading to other parts of the body. Melanomas that have spread to areas besides the skin are called Metastatic Melanomas
- The primary site of origin could be the skin/mucous membrane (lining of the gastrointestinal tract)/eye.
- Stage III Melanomas have metastasized to local lymph nodes
- Stage IV Melanomas have metastasized to internal organs
- The organs commonly involved in metastasis (spread) include:
- Brain
- Liver
- Lungs
- Bone
- Brain metastases tend to be aggressive and are difficult to treat.
- Metastatic Melanoma maybe diagnosed with a biopsy of the suspicious areas, but more often require imaging scans such as MRI or CT of the affected regions as well
- A combination of drugs and/or surgery, or radiation, is required for treatment of the condition, although the outcomes are often poor
Who gets Metastatic Melanoma? (Age and Sex Distribution)
- Primary Cutaneous Melanoma can occur in young as well as old individuals, and is one of the most common cancers in people younger than 30 years
- In the United States, it has been observed that women are at increased risk before the age of 40 years, while men are at a higher risk after the age of 40 years
- Metastatic Melanoma can occur in any age or gender who have had a primary melanoma
What are the Risk Factors for Metastatic Melanoma? (Predisposing Factors)
Melanomas of skin/eyes or other locations are capable of spreading to other sites, leading on to Metastatic Melanomas. Any factor that increases the risk of these tumors therefore, increases the risk of metastasis as well. Some of the risk factors include:
- Exposure to ultra violet (UV) rays is a major risk factor. UV rays are present in sunlight, and also in tanning lamps and beds
- Nevus (medical term for mole) is a non-cancerous pigmented tumor. While most nevi never become cancerous (or malignant), a small number of atypical/dysplastic nevi (moles with abnormal shape/borders/color) may turn cancerous. When such dysplastic nevi run in families, the condition is called dysplastic nevus syndrome. Individuals with this condition have a 10% increased risk of developing melanoma. Despite the above and irrespective of the condition, whether the nevi are present since birth, or are normal, or atypical; more the number of moles, more is the risk
- Fair-skinned individuals are at a higher risk; more so those with freckles or those who develop sun burns, easily
- Previous history of melanoma or a history of melanoma in parents/siblings
- An inherited condition called xeroderma pigmentosum, where the ability of the cells to repair sun-induced damage to genetic material is impaired
- Weakened immune system, as a result of infections (like HIV), drugs (chemotherapy or immunosuppressants), and due to the presence of cancers (like lymphoma)
- Individuals with advanced primary melanomas (at the site of origin), or those with melanomas that have been left untreated (or partially treated), are at increased risk of developing metastatic disease
When the primary tumor is located on the head, neck, trunk, or abdomen, and ulceration (with open sore) is noted, then the risk for brain metastasis increases. About 60% of individuals with Stage IV Melanoma will develop brain metastasis.
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases one’s chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Metastatic Melanoma? (Etiology)
While the exact cause behind melanomas is yet to be determined, melanoma of the skin is better understood compared to that of the eye or other locations. The exact reason why some moles turn cancerous, and others do not, is still not well-understood. However, the potential causes for melanoma include:
- Uncontrolled activity of oncogenes (rogue genes that promote cell growth and division) or depressed action of tumor suppressor genes (genes that normally keep a check on cell growth and division) is thought to play a role in development of melanomas.
- About 50% of all melanomas have a mutation (change) involving the BRAF oncogene.
- UV radiation induces damage to DNA (the genetic material that determines all of our traits and functions) and this in turn may turn on oncogenes or turn off tumor suppressor genes
- Ocular (eye) melanomas may be caused by changes involving GNA11 and GNAQ oncogenes, or BAP 1 tumor suppressor gene
Whatever be the site of origin, the tumor cells eventually spread to other areas via blood or tissue fluid (lymph), leading on to Metastatic Melanoma.
What are the Signs and Symptoms of Metastatic Melanoma?
The signs and symptoms of Metastatic Melanoma include those caused by the primary (original) tumor and those produced by spread (metastasis). The primary tumor (at site of origin) may be:
- A pigmented area on the skin that is Asymmetrical/has irregular Borders/not uniformly Colored/has a Diameter more than ¼ inch (6 millimeters) or appears to be changing in shape or color over time (Evolving). These are often referred to as the ABCDE characteristics of melanoma by physicians. (Source: The Skin Cancer Foundation, New York)
- A suspicious area may also develop redness, swelling, or develop open sores (ulcers), or may show ooze of fluid, or blood
- Ocular melanoma (melanoma of the eye) can start out as a spot on the iris (the colored part of the eyeball)
- Metastatic Melanoma may present with non-specific symptoms like fatigue, loss of weight, loss of appetite, nausea, and further symptoms related to the organs that are involved. These are highly variable and may include symptoms like headache, vomiting, seizures, bone pain, aches, jaundice, etc.
- In rare cases, when the melanoma spreads very early, the organ specific symptoms may predominate, while the primary tumor (at site of origin) is still small.
- Uncommonly, Metastatic Melanoma may be detected without finding melanoma anywhere on the body. In these cases, a prior melanoma regressed in response to immune system response, with the destruction of the primary melanoma not preventing the Metastatic Melanoma component may be noted
How is Metastatic Melanoma Diagnosed?
A thorough history and a complete physical exam by a physician are crucial for the diagnosis of Metastatic Melanoma. This is followed by some tests which include:
- Biopsy of skin: A sample of the skin, from any suspected area found on physical examination, is taken and examined under a microscope for signs of cancer by a pathologist. The types of biopsy performed include:
- Excisional biopsy: After numbing the area with a local anesthetic, the entire mole is removed with a small border of surrounding skin. Where possible, this is the generally preferred method
- Punch biopsy: After numbing the area with a local anesthetic, a circular blade is pressed into the skin around the suspicious area, and a round piece of skin removed. This type of biopsy is carried out, when the lesion (the suspicious area) is large in size
- Incisional biopsy: After numbing the area with a local anesthetic, a portion of the tumor is removed using a surgical knife
- To detect lymph nodal spread:
- Sentinel lymph node biopsy: Performed to determine if the melanoma has spread to nearby lymph nodes. A dye is injected into the area from where the melanoma is removed. The first lymph node that takes up the dye is biopsied and examined for cancer cells, under a microscope
- If any lymph node can readily be felt on physical exam, biopsy is carried out using the fine needle aspiration cytology (FNAC) technique. In this, a sample of cells is removed from the mass, using a syringe with a hollow needle and then examined under a microscope
- Imaging studies may be done to detect spread to other organs. This may include
- Chest x-rays
- CT/MRI scan of the affected regions
- Biopsy of samples from organs maybe needed in some cases, to determine the type of cancer; especially, when a skin lesion is not found
- Blood tests: Blood levels of a substance called LDH (lactate dehydrogenase) are determined. Increased levels of LDH, indicate that the tumor has spread to internal organs
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of Metastatic Melanoma?
With Metastatic Melanoma, the cancer cells have spread to involve the lymph nodes and organs. Organ metastases can lead to organ specific damage.
How is Metastatic Melanoma Treated?
A combination of therapies is required to treat Metastatic Melanoma. Treatment options include:
Drug therapy:
- Immunotherapy
- This therapy stimulates the immune system and involves the use of substances produced naturally by the body or such similar synthetics, made in a laboratory
- Drugs used include, synthetic immune proteins and proteins that boost the immune system, called interleukin-2
- Synthetic immune proteins may cause the immune system to start attacking other parts of the body. Interleukin-2, besides causing flu-like symptoms, in high does may also cause serious side effects, including irregular heart rhythms, low blood pressure, and fluid accumulation in the lungs
- Targeted therapy
- Involves the use of drugs tailored to target the differences in a melanoma cell, as compared to a normal cell
- Half of all melanomas involve a mutation in the BRAF gene. This is targeted by a drug vemurafenib and trametinib
- Side effects may include nausea, joint pain, fatigue, rash, itching, hair loss, sensitivity to the sun, and rarely heart rhythm problems, liver problems, severe allergic reactions, and severe skin or eye problems
- Chemotherapy
- Drugs are used to kill the tumor cells, which may be given as oral pills, or injected into veins
- Side effects of chemotherapy may include nausea, vomiting, hair loss, loss of appetite, diarrhea, and fatigue, increased risk of infection, mouth sores, or easy bruising, depending on the drug used
- In cases, where the melanoma is advanced, but remains confined to an arm or leg; chemotherapy is only circulated through the affected the limb, by a process called isolated limb perfusion
Surgery:
- If the melanoma has spread to a very limited number of sites, surgery may be recommended. However, this is rarely curative, because Metastatic Melanoma usually spreads to many body regions, sometimes throughout the body
- Surgery may help in reducing the size of the tumor at the site of origin. It may also relieve pain caused by a metastatic tumor, such as in the lung or brain
- Lymph node dissection maybe performed, if any nodal spread is detected
Radiation therapy:
- This uses high energy beams to kill cancer cells
- It is especially useful in brain metastases, or if multiple tumors are present, or if tumors are present in a site inaccessible to surgery
- The most common side effect is fatigue, but this gets resolved, once the treatment is complete
Palliative therapy: The aim of palliative therapy is to improve the quality of life in terminally ill individuals. The mainstay of this therapy is pain-relief and relief of other symptoms that cause discomfort.
If the melanoma has been completely treated, regular physician visits every 3-6 months for 2 years is necessary. This should be followed by visits every 3-12 months for the next few years, after which annual visits are a must. In other situations, the frequency of visits maybe tailored specifically, based on the healthcare provider’s advice.
How can Metastatic Melanoma be Prevented?
Early diagnosis and treatment of melanoma is crucial in the prevention of Metastatic Melanomas. Steps adopted to prevent melanoma, also help in prevention of the metastatic form. These include:
- Avoid direct exposure to UV rays and remain in the shade, as and when possible
- When heading out into the sun:
- Slip on a shirt
- Slop on some sunscreen. Sunscreens with SPF values higher than 30, and those offering broad spectrum protections (against UV-A and UV-B rays), are recommended. Apply an ounce to all exposed areas, 30 minutes before heading outdoors. Reapply every two hours, and also after excessive sweating
- Slap on a hat
- Wrap on sunglasses
This is encapsulated as the “Slip! Slop! Slap! Wrap” method for skin cancer prevention. (Source: The American Cancer Society, Atlanta)
- Avoid tanning beds and sun lamps
- Perform self-examination of your skin, from head to toe, once a month
- Get a professional skin exam from a healthcare provider, once a year
- All patients with melanoma should undergo skin examinations regularly even after treatment, at least once a year throughout their lives. The frequency of follow-up is determined by the healthcare provider and is a must, to detect any new tumors, or recurrences, or spread of melanoma, as early as possible
What is the Prognosis of Metastatic Melanoma? (Outcomes/Resolutions)
- The outcomes of Metastatic Melanomas are, in general, poor with only 15-20% of the patients surviving the initial period of 5 years following detection; 10-15% may survive up to 10 years. The prognosis is however better, with normal levels of LDH
- Brain metastasis carries a poor prognosis
The prognosis depends upon a set of several factors, which include:
- Stage of tumor: With lower-stage tumors, when the melanoma is confined to site of origin, the prognosis is usually excellent with appropriate therapy. In higher-stage cancers, such as those with metastasis, the prognosis is poor
- Overall health of the individual: Individuals with overall excellent health have better prognosis compared with those with poor health
- Age of the individual: Older individuals generally have poorer prognosis than younger individuals
- The size of the melanoma: Individuals with small-sized melanomas fare better than those with large-sized ones
- Individuals with bulky disease have a poorer prognosis
- Involvement of vital organs may complicate the condition
- The surgical resectability of Metastatic Melanoma (meaning if the melanoma can be removed completely) - which is a very rare option
- Whether the cancer is occurring for the first time or is recurrent. Recurring cancers have worse prognosis compared to those that do not recur
- Response to treatment: Melanomas that respond well to treatment have better prognosis compared to melanomas that do not respond to treatment
- Progression of the condition makes the outcome worse
An early diagnosis and prompt treatment of the condition generally yields better outcomes than a late diagnosis and delayed treatment.
Additional and Relevant Useful Information for Metastatic Melanoma:
- The brain has a defense mechanism against the penetration of harmful substances, called the blood brain barrier. These barriers reduce the entry of medications into the brain, as well as make brain metastasis, difficult to treat
- Mucosal melanomas should not be confused with Metastatic Melanomas. A Metastatic Melanoma usually occurs from a melanoma of the skin or eye. Mucosal melanomas of internal organs of the body, such as gallbladder, intestines, urinary bladder, etc. are considered primary melanomas meaning that they originate from the primary site
- In many cases, if mucosal melanomas are not diagnosed early, they can spread to other organs. When they spread from their site of origin to other locations, then they are called Metastatic Melanomas of mucosal melanomas

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.