What are the other Names for this Condition? (Also known as/Synonyms)
- Mucinous Bronchioalevolar Carcinoma of Lung
- Mucinous Bronchoalevolar Carcinoma of Lung
- Pulmonary Invasive Mucinous Adenocarcinoma
What is Invasive Mucinous Adenocarcinoma of Lung? (Definition/Background Information)
- Invasive adenocarcinoma of lung is the most commonly diagnosed type of lung cancer. It is a type of non-small cell lung cancer that usually develops in the peripheral region of the lungs (peripheral airways). It can be broadly subdivided into invasive mucinous adenocarcinoma and invasive non-mucinous adenocarcinoma
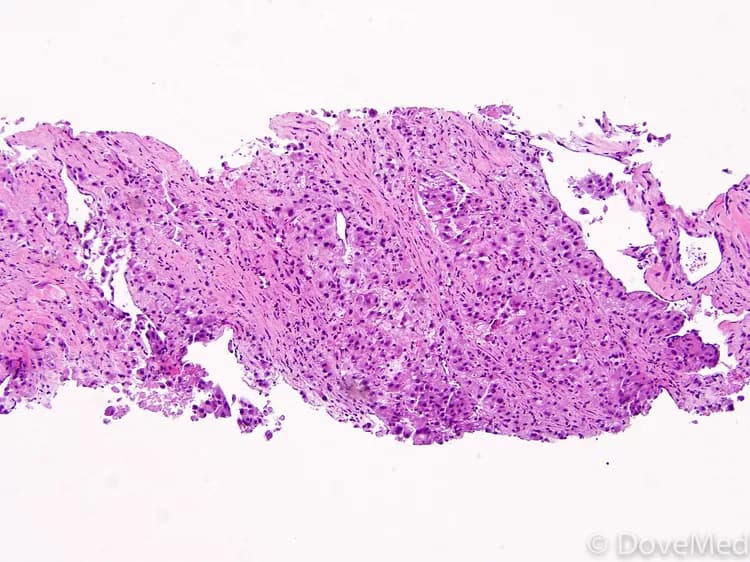
- Invasive Mucinous Adenocarcinomas of Lung form a new category of tumors. These were formerly categorized as mucinous bronchioalevolar carcinoma. The tumor is diagnosed under a microscope, on examination of the cancer cells by a pathologist
- The Invasive Mucinous Adenocarcinoma of Lung can have any histological pattern; the most common pattern noted is lepidic. Other patterns that may be present include the papillary, micropapillary, or acinar; however, the solid pattern is generally not noted
- The cause of Invasive Mucinous Adenocarcinoma of Lung is generally unknown, but it is influenced by smoking. Even though mostly tobacco smokers are affected, Lung Adenocarcinomas form the largest subset of lung cancers observed in non-smokers (and are mostly women)
- Invasive Mucinous Adenocarcinoma of Lung can cause chest pain, breathing difficulties, fatigue, and other general signs and symptoms, such as fever, weight loss, and appetite loss
- Chemotherapy, surgery, radiation therapy, and other treatment measures may be used for treating Invasive Mucinous Adenocarcinoma of Lung based on the assessment of the physician
- The prognosis depends on many factors including the subtype, grade and stage of the tumor, progression of the condition, response to treatment, and overall health of the individual. In general, the prognosis of Invasive Mucinous Adenocarcinoma of Lung is guarded
Who gets Invasive Mucinous Adenocarcinoma of Lung? (Age and Sex Distribution)
- Individuals under the age of 40 years are rarely diagnosed with lung cancer. The majority of Invasive Mucinous Adenocarcinoma of Lung cases are detected and diagnosed in adults over the age of 65 years
- Both males and females are affected
- Current studies do not show any racial or ethnic predilection
What are the Risk Factors for Invasive Mucinous Adenocarcinoma of Lung? (Predisposing Factors)
There are no specific risk factors that have been identified for Invasive Mucinous Adenocarcinoma of Lung. Although, in general, physicians believe that certain factors may increase an individual’s risk for lung cancers and these include:
- Advancing age: The risk increases with age and most cases occur in individuals over the age of 65 years
- Smoking: Smoking cigarettes, cigars, or pipes, increase the risk due to damaging chemicals being inhaled into the lungs. Prolonged smoking damages the lung, resulting in reduced clearance of the chemical carcinogens that accumulate in the lungs. This can lead to an increased risk of developing lung cancer
- Exposure to secondhand smoke: Individuals, who do not smoke, but live with smokers, also have an increased risk
- Air pollution: Exposure to polluted air may increase any individual’s risk. This is true, especially in the case of smokers, who are exposed to air pollution, than non-smokers
- Exposure to asbestos and other harmful chemicals: Prolonged exposure to asbestos and other harmful chemicals including arsenic, chromium, nickel, and tar
- Radon causing indoor air pollution: Radon, a colorless, odorless, and tasteless radioactive gas is produced by the natural breakdown of uranium in soil and rocks. In certain geographical regions, hazardous levels of radon gas can develop inside building or households. Individuals exposed to excessive amounts of radon gas are vulnerable to lung cancer
- Family history: Individuals with one or more immediate family members or relatives with a history of lung cancer
- Personal history: Individuals who have previously had lung cancer have an increased risk of its recurrence
- Certain longstanding lung diseases: Lung diseases, such as lung fibrosis, tuberculosis, bronchitis, or chronic obstructive pulmonary disease (COPD) over a prolonged period of time, may increase an individual’s risk
- Radiation therapy to the chest: Individuals who had radiation therapy to the chest for another cancer are increasingly prone to lung cancer
- Working in mines
- The presence of alpha 1 antitrypsin deficiency disorder
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases ones chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Invasive Mucinous Adenocarcinoma of Lung? (Etiology)
The exact cause of Invasive Mucinous Adenocarcinoma of Lung is unknown.
- However, it is believed that there are certain factors contributing to the condition, which include smoking, exposure to radon, and prolonged exposure to asbestos and other harmful chemicals (arsenic, chromium, nickel, and tar)
- Lung adenocarcinomas have been shown to have a variety of different genetic mutations. This includes the involvement of ALK, KRAS, and EGFR genes. The frequently involved gene in the case of mucinous adenocarcinoma type is the KRAS gene (in 90% of the cases)
- Gene fusion involving the NRG1 gene has been recently discovered and is being researched upon
- In general, it is known that cancers form when normal, healthy cells begin transforming into abnormal cells - these cancer cells grow and divide uncontrollably (and lose their ability to die), resulting in the formation of a mass or a tumor
- The transformation of normally healthy cells into cancerous cells may be the result of genetic mutations. Mutations allow the cancer cells to grow and multiply uncontrollably to form new cancer cells
- These tumors can invade nearby tissues and adjoining body organs, and even metastasize and spread to other regions of the body
What are the Signs and Symptoms of Invasive Mucinous Adenocarcinoma of Lung?
Early-stage lung cancer rarely causes any signs and symptoms and initially makes for a difficult diagnosis. Besides, several of the primary symptoms may result from non-malignant disorders too. The overlapping signs and symptoms may result in a delayed diagnosis of lung cancer in some cases.
The common signs and symptoms may include the following:
- Shortness of breath that gets worse with time; difficulty in breathing
- Cough that may be persistent; blood in cough/sputum (hemoptysis)
- Chest pain, heaviness in the chest
- Changes to voice, hoarseness, or loss of voice
Signs and symptoms associated with Invasive Mucinous Adenocarcinoma of Lung, which may emerge during the later stages of the condition, include:
- High temperatures (fever) and excessive night sweats (may be recurrent)
- Sudden weight loss; unintentional weight loss; changes in appetite
- The individual is easily tired, resulting in fatigue even with minimal activity
- Headache
- Low blood pressure
- Bronchorrhea (watery sputum production)
Paraneoplastic syndrome associated symptoms:
- These are a set of signs and symptoms that occur in the body due to the presence of cancer, due to changes in the immune system
- Paraneoplastic and endocrine syndrome is commonly observed in lung cancer, but to a lesser extent in lung adenocarcinoma (compared to other histological subtypes)
- Paraneoplastic symptoms can also occur due to brain involvement leading to neurological signs and symptoms. These may be seen many months before lung cancer is diagnosed
Some features of the tumor include:
- These mucinous adenocarcinomas are mostly invasive; they originate from many points (multicentric), are multilobar, and spread through the air cavities within the lungs (aerogenous spread)
- A majority of the tumors originate from the smaller airways (peripheral lung); the upper lobes are mostly affected. However, tumors may be present anywhere in the lung
- Both lungs are usually affected
- Adenocarcinomas of lung can be solitary tumors, or appear as multiple nodules; the size of the tumor may differ widely. There may also be a primary tumor with satellite smaller-sized tumors
- Some tumors are diffuse and widespread; while others appear as multiple nodules that are clumped together
- In later stages, these are known to invade into the pleura
How is Invasive Mucinous Adenocarcinoma of Lung Diagnosed?
The following procedures and tools may be used in the diagnosis of Invasive Mucinous Adenocarcinoma of Lung:
- Physical examination: During a physical exam, a physician will check the individual’s overall health status, listen to their breathing, and check for possible fluid buildup in the lungs (auscultation)
- Pulmonary function tests can help determine the extent of lung damage; it can also help the healthcare provider assess the ability of lungs to deliver oxygen to the body
- Chest X-ray: Two-dimensional pictures using tiny amounts of radiation are taken, in order to detect any tumors or other medical issues associated with the lungs, such as pneumonia. Tumors inside the lung can be detected using a chest X-ray; although sometimes, these tumors are too small to visualize (tumors less than 1 cm in size may be missed on a chest X-ray)
- Computerized tomography (CT) scan: Also known as CAT scan, this radiological procedure creates detailed three-dimensional images of structures inside the body. CT scans may be helpful in detecting recurrences, or if the cancer has metastasized to the surrounding lymph nodes of the lungs
- Magnetic resonance imaging (MRI) scan: An MRI scan uses magnetic fields that create high quality pictures of certain body parts, such as tissues, muscles, nerves, and bones. These high-quality images may indicate to a physician, if any tumor is present
- Positron emission tomography (PET): A PET scan is a nuclear medicine imaging technique that uses three-dimensional images to show how tissue and organs are functioning. A small amount of radioactive material may be injected into a vein, inhaled or swallowed. A PET scan is also helpful in detecting recurrences, or if any metastasis (to the surrounding lymph nodes of the lungs) has occurred
- Sputum cytology: Sputum cytology is test that involves the collection of mucus (sputum), coughed-up by a patient. After the mucus is collected, a pathologist examines it in an anatomic pathology laboratory, to see if any cell abnormalities are present indicative of Pulmonary Adenocarcinoma
- Bone scan: A bone scan is a nuclear imaging test that involves injecting a radioactive tracer into an individual’s vein. Bone scans are primarily used to detect if the cancerous cells have metastasized to the bones and formed secondary tumors
- Bone marrow biopsy: Bone marrow is a soft tissue found within bones. Occasionally, with Adenocarcinoma of Lung, a bone marrow biopsy is used to detect blood abnormalities, or if a physician believes that metastasis to the bone marrow may have occurred
A biopsy refers to a medical procedure that involves the removal of cells or tissues, which are then examined by a pathologist. Different biopsy procedures include:
- Tissue biopsy from the affected lung:
- A biopsy of the tumor is performed and sent to a laboratory for a pathological examination. A pathologist examines the biopsy under a microscope. After putting together clinical findings, special studies on tissues (if needed) and with microscope findings, the pathologist arrives at a definitive diagnosis. Examination of the biopsy under a microscope by a pathologist is considered to be gold standard in arriving at a conclusive diagnosis
- Biopsy specimens are studied initially using Hematoxylin and Eosin staining. The pathologist then decides on additional studies depending on the clinical situation
- Sometimes, the pathologist may perform special studies, which may include immunohistochemical stains, molecular testing, flow cytometric analysis and very rarely, electron microscopic studies, to assist in the diagnosis
- The biopsy may be performed through any of the following procedures:
- Bronchoscopy: A special medical instrument, called a bronchoscope, is inserted through the nose and into the lungs to collect small tissue samples
- Thoracentesis: During thoracentesis, physicians use a special medical device called a cannula, to remove fluid between the lungs and the chest wall for examination
- Thoracoscopy: A medical instrument called a thoracoscope is inserted into the chest through tiny incisions, in order to examine and remove tissue from the chest wall, which is then analyzed further
- Thoracotomy: Thoracotomy is a surgical invasive procedure with special medical instruments to open-up the chest and remove tissue from the chest wall or the surrounding lymph nodes of the lungs
- Mediastinoscopy: A medical instrument called a mediastinoscope is inserted into the chest wall to examine and remove samples
- Fine needle aspiration biopsy (FNAB) or transthoracic needle biopsy: A device called a cannula is used to extract tissue or fluid from the lungs, or surrounding lymph nodes
- Open lung biopsy
A differential diagnosis with respect to other lung cancer types may be necessary prior to establishing a definite diagnosis, by excluding the following cancers:
- Adenocarcinoma in situ of the lung
- Minimally invasive adenocarcinoma of the lung
- Secondary lung tumors that have metastasized from other regions to the lung
- Metastatic tumors from ovary or pancreas that resemble lung adenocarcinomas
- Colorectal adenocarcinoma that has metastasized to the lung
Note:
- In a majority, pure forms are not seen and the tumor is often heterogeneous (with a mix of more than one subtype)
- The tumors are classified as mixed invasive mucinous adenocarcinomas, if more than 10% of any other histological component is present
- An accurate diagnostic evaluation is crucial for staging purposes
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of Invasive Mucinous Adenocarcinoma of Lung?
The complications of Invasive Mucinous Adenocarcinoma of Lung can include:
- Dyspnea (shortness of breath): If the cancerous tumor expands to block important, large, or small airways of the chest or lung
- Hemoptysis (coughing-up blood): Individuals may cough-up blood, due to excessive amounts of blood in the airways
- Pain: Advanced stages that has metastasized to the pleural cavity (lining surrounding the lungs), invaded the chest wall, or other areas of the body may cause excessive pain
- Involvement of local and distant organs in lung cancer: Loss of function of the organ/area to which cancer has spread or metastasized, due to systemic involvement
- Pleural effusion (fluid in the chest): Excessive fluid accumulation, resulting from cancerous cells spreading inside the lungs, or outside of the lungs
- Irreversible lung damage such as due to lung fibrosis
- Development of pneumothorax (collapsed lung)
- Paraneoplastic symptoms can also occur with recurrences - such symptoms may be an indicator of relapse
- Recurrence following surgical removal of the tumor; this is less frequently observed with adenocarcinomas
There may be complications related to the methods used in treating the condition and may include:
- Side effects of radiation therapy that may include sunburn-like rashes, where radiation was targeted, red or dry skin, heaviness of the breasts, and general fatigue
- Side effects of chemotherapy, which may include nausea, vomiting, hair loss, decreased appetite, mouth sores, fatigue, low blood cell counts, and a higher chance of developing infections
- The treatment can also cause infertility in men and women. Hence, measures to protect the individual’s fertility must be considered, before starting chemotherapy
How is Invasive Mucinous Adenocarcinoma of Lung Treated?
Treatment options available for individuals with Invasive Mucinous Adenocarcinoma of Lung are dependent upon the following:
- Type of cancer
- Location of the cancer
- The staging of the cancer: If lung cancer is diagnosed, staging helps determine whether it has spread and which treatment options are best-suited for the individual
- Personal preferences
- Overall health status of the individual
- Type of gene mutation involved: This factor can determine the treatment possibilities or relative treatment resistance
The most commonly used treatment is surgery. Surgery can be potentially curative, if the tumor is completely excised (in case of lower stage tumors). However, some cases show recurrence many years later. Chemotherapy and radiation may also be used for treatment, if surgery is not a viable option, or if there is a suspicion of metastasis.
Surgery: Depending on the stage of Invasive Mucinous Adenocarcinoma of Lung, surgery might be a viable option. However, the location of the tumor in the periphery makes it commonly associated with metastasis. The surgical options include:
- Wedge resection: Wedge resection is a partial removal of the wedge-shape portion of the lung that contains cancerous cells (along with any surrounding healthy tissue)
- Segmentectomy: It is the partial removal of the cancerous lung and any surrounding healthy tissue
- Pulmonary lobectomy: It is a type of surgical procedure performed to partially remove a portion of a lung
- Sleeve lobectomy: It is another surgical procedure to partially remove a portion of the lung and a part of the airway (bronchus)
- Pneumonectomy: It is the surgical removal of the entire lung
Chemotherapy:
- Chemotherapy drugs are typically taken as pills, or injected directly into a vein. These drugs travel through the body to kill any cancer cells
- But, they can also kill healthy cells, located within the gastrointestinal tract and in hair follicles. The side effects include vomiting, nausea, and hair loss
Radiation therapy:
- Radiation therapy involves using x-rays to kill cancerous cells. High-powered radiation beams are directed to particular body regions to target cancer. In the process, healthy cells can also be damaged
- Radiation therapy can be administered in the following ways:
- Either by a machine, placed outside the body (called external beam radiation)
- Or it may be administered internally, by a device positioned directly at, or close to the malignant tumor, inside the lungs (called brachytherapy)
Radiation therapy and chemotherapy can be used as a combination therapy. Combinational therapy increases the effects of both types of treatment. However, the side effects are cumulative.
Targeted drug therapy: Targeted drug therapy is a relatively new medical treatment used to target abnormal cancer cells and reduce the chance of cancer spreading to other parts of the body.
How can Invasive Mucinous Adenocarcinoma of Lung be Prevented?
Currently, there is no known prevention method for Invasive Mucinous Adenocarcinoma of Lung. Although there are no preventable measures for lung cancer, in general, various steps can be taken to help decrease the risk of its formation. These measures include:
- Complete smoking cessation and avoiding exposure to secondhand smoke: The risk for lung cancer decreases drastically following quitting or giving up smoking
- Physical activity: Individuals, who participate in a moderate amount of physical activity, may decrease their risk
- Adequate consumption of fruits and vegetables: A healthy diet, low in saturated fats and rich in many fruits and vegetables, may help decrease one’s risk for lung cancer
- Avoid exposure to certain materials and chemicals (including asbestos, arsenic, chromium, nickel, and tar): Individuals who work with such substances should follow proper usage principles and occupational safety instructions, since a prolonged exposure to harmful chemicals may increase the risk for lung cancer. This risk is multiplied in smokers who are exposed to these harmful chemicals
- Avoid exposure to radioactive gas: Radon, a radioactive gas, produced by the natural breakdown of uranium in soil and rocks, may develop to hazardous levels inside building spaces. Individuals exposed to excessive amounts of radon gas are vulnerable to lung cancer
- Limit alcohol consumption: Alcoholic beverages have been linked to increasing an individual’s risk for certain types of cancers, such as those affecting the lungs, mouth, throat, esophagus, breast, colon, and liver
- CT screening in high-risk groups can decrease the incidence of lung cancer, or at least help detect such cancers early. A low-dose CT scan is good to identify adenocarcinomas early. It is generally known that CT scans are about 3-4 times better than X-ray studies
What is the Prognosis of Invasive Mucinous Adenocarcinoma of Lung? (Outcomes/Resolutions)
- Invasive Mucinous Adenocarcinoma of Lung is a type of invasive malignancy. The prognosis of the condition is generally guarded, since the tumors are aggressive. However, it is also dependent upon the proportion of the histologic subtype and stage of the cancer during diagnosis among various other factors
- The prognosis of lung cancer, in general, depends upon a set of several factors that include:
- The grade of the lung tumor such as grade1, grade2, and grade 3. Grade1 indicates a well-differentiated tumor, grade 2 a moderately-differentiated tumor, whereas grade 3 indicates a poorly-differentiated tumor. Grade 3 tumors are higher prone to metastasis to the lymph nodes and recurrences
- Stage of lung cancer: With lower-stage tumors, when the tumor is confined to site of origin, the prognosis is usually excellent with appropriate therapy. In higher-stage tumors, such as tumors with metastasis, the prognosis is poor
- Histological subtype of the tumor: Some subtypes have better prognosis than others
- The size of the lung tumor: Individuals with small-sized tumors fare better than those with large-sized tumors
- Overall health of the individual: Individuals with overall excellent health have better prognosis compared with those with poor health
- Age of the individual: Older individuals generally have poorer prognosis than younger individuals
- Individuals with bulky disease of the lung cancer have a poorer prognosis
- Involvement of the lymph node, which can adversely affect the prognosis
- Involvement of vital organs may complicate the condition
- The surgical respectability of the tumor (meaning, if the tumor can be removed completely)
- Whether the tumor is occurring for the first time, or is a recurrent tumor. Recurring tumors have worse prognosis compared to tumors that do not recur
- Response to treatment of lung cancer: Tumors that respond to treatment have better prognosis compared to tumors that do not respond to treatment
- Progression of the condition makes the outcome worse
- An early diagnosis and prompt treatment of the tumor generally yields better outcomes than a late diagnosis and delayed treatment
- The combination chemotherapy drugs used, may have some severe side effects (like cardio-toxicity). This chiefly impacts the elderly adults, or those who are already affected by other medical conditions. Tolerance to the chemotherapy sessions is a positive influencing factor
It is important to have follow-up appointments with a physician, to evaluate the effects of the current treatment method, and to monitor for any returning tumors.
Additional and Relevant Useful Information for Invasive Mucinous Adenocarcinoma of Lung:
- Lung cancer incidence is around 35 cases per 100,000 populations: The incidence of lung cancer in non-smokers is 1-2 cases per 20,000 populations per year; its incidence in smokers is 20-30 times higher than that of non-smokers
- Studies under WHO indicate that the number of adenocarcinoma of lung cases is increasing (or has increased) due to design changes to cigarettes, composition of certain contents, and even better filtration of smoke through the cigarette. This is researched to be due to increased nitrosamines being inhaled through tobacco smoke

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.