What are the other Names for this Condition? (Also known as/Synonyms)
- Dextro-Looped Transposition of the Great Arteries (DTGA)
- DTGA (Dextro-Looped Transposition of the Great Arteries)
- TGA (Transposition of the Great Arteries)
What is D-Transposition of the Great Arteries? (Definition/Background Information)
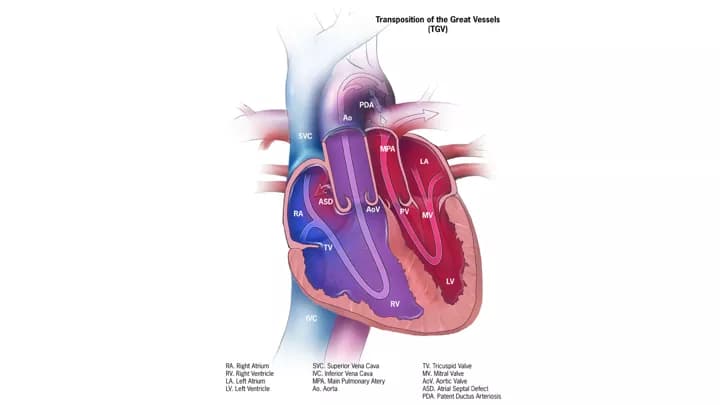
- Congenital heart defects are relatively common birth defects involving the heart, and these may be of several types. Dextro-Transposition of the Great Arteries (d-TGA) is a congenital heart abnormality in which the aorta and the pulmonary artery are transposed (i.e., their normal connections are reversed)
- Normally there are two blood vessels, the aorta and the pulmonary artery that come out of the heart. The function of the pulmonary artery is to carry oxygen-poor blood to the lungs; the aorta is responsible for carrying oxygen-rich blood to the rest of the body
- In D-Transposition of the Great Arteries, oxygen-rich blood from the lungs is pumped back into the lungs, and oxygen-deficient blood is circulated to the body. The cause of development of this heart defect is not well understood. A positive family history may be a risk factor for d-TGA
- Newborn babies with D-Transposition of the Great Arteries have acute respiratory issues (breathing difficulties) and present severe blue discoloration of the skin. This condition is classified as a critical congenital heart defect (CCHD) requiring immediate treatment, including surgical correction of the defect
Who gets D-Transposition of the Great Arteries? (Age and Sex Distribution)
- D-Transposition of the Great Arteries is a rare congenital disorder that occurs in approximately 3% of all congenital heart defect cases
- The incidence of the condition is estimated at 1 in 3,400 live births
- The presentation of symptoms are apparent at birth
- Both males and females may be affected
- Worldwide, individuals of all racial and ethnic groups may be affected
What are the Risk Factors for D-Transposition of the Great Arteries? (Predisposing Factors)
- A positive family history may be an important risk factor, since D-Transposition of the Great Arteries can run in families
- Currently, no other risk factors have been clearly identified for the disorder
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases one’s chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of D-Transposition of the Great Arteries? (Etiology)
Presently, the exact cause of D-Transposition of the Great Arteries (d-TGA) is not known. It may develop from a combination of factors that may be genetic and environmental. It is also believed that what the expectant mother consumes, such as food, drink, or even some medications, may be contributive.
- Most cases of TGA develop sporadically, during the development of the fetal heart, which occurs in the first 8 weeks of development
- A genetic basis for the condition may exist since it is known to run in families. The exact gene mutation that leads to d-TGA and the mode of inheritance are not known
- Children with d-TGA are also seen to have other cardiac anomalies, typically atrial septal defect or ventricular septal defect
What are the Signs and Symptoms of D-Transposition of the Great Arteries?
The signs and symptoms of D-Transposition of the Great Arteries are generally noted within the first few days/weeks of life. It may include:
- Cyanosis (skin is blue-tinged), which may be severe
- Skin that feels cold and clammy
- Rapid and shallow breathing
- Labored breathing
- Elevated heart rate
- Poor feeding and irritability
How is D-Transposition of the Great Arteries Diagnosed?
D-Transposition of the Great Arteries is diagnosed on the basis of the following information:
- Complete physical examination and thorough medical and family history evaluation
- Assessment of the signs and symptoms, particularly pale skin of the child, breathing difficulties, pounding heart, and irritability
- Through heart examination to observe any abnormalities such as irregular heartbeat
- Newborn pulse oximetry screening may help the healthcare suspect the condition prior to symptom presentation
- Electrocardiogram (EKG), to measure electrical activity of the heart
- Echocardiogram may be performed on the fetus to detect any coarctation; it is commonly used to confirm the diagnosis
- Chest X-ray
- CT and MRI scan studies of the chest and abdomen
- Cardiac catheterization, to obtain a clear image of all the four chambers of the heart and the great vessels
- Prenatal screening tests
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of D-Transposition of the Great Arteries?
The complications of D-Transposition of the Great Arteries may include:
- Respiratory distress
- Cardiac arrest, without treatment
Complications may occur with or without treatment, and in some cases, due to treatment also, and may include:
- Right ventricular dysfunction
- Leaks and obstruction in cardiac valves
- Elevated or reduced heart rates
- Pulmonary hypertension
Children may present lifelong complications following surgical correction of the abnormality.
How is D-Transposition of the Great Arteries Treated?
The treatment for D-Transposition of the Great Arteries (d-TGA) may include the following:
- Oxygen supplementation to ease breathing
- Cardiac catheterization and balloon atrial septostomy to improve heart function
- Surgical repair of transposition - surgery is mandated in all cases of d-TGA and may be any of the following two types:
- Arterial switch operation: This is the most commonly performed invasive procedure, and is frequently undertaken within the first 30 days of birth
- Atrial switch operation: This surgical repair procedure is performed only in some cases
- Post-surgery, medications are prescribed to regulate blood pressure, remove extra fluids from the body, and help the heart pump better
- Pacemaker implantation surgery may be needed in some cases (later)
A lifelong follow up with a cardiologist will be required for infants who undergo corrective surgery, in order to monitor the heart function.
How can D-Transposition of the Great Arteries be Prevented?
Presently, D-Transposition of the Great Arteries is not a preventable condition.
- If there is a family history of the condition, then genetic counseling will help assess risks, before planning for a child
- Active research is currently being performed to explore the possibilities for treatment and prevention of such congenital heart conditions
What is the Prognosis of D-Transposition of the Great Arteries? (Outcomes/Resolutions)
- The prognosis of D-Transposition of the Great Arteries is good with prompt surgical treatment. Most babies recover and exhibit normal patterns of growth and development
- However, some individuals may develop complications as a result of surgery, which may last a lifetime. Regular check-ups are necessary to monitor the health of such individuals
Additional and Relevant Useful Information for D-Transposition of the Great Arteries:
The following DoveMed website link is a useful resource for additional information:

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.