What are the other Names for this Condition? (Also known as/Synonyms)
- AD (Alzheimer’s Disease)
- Alzheimer Disease
- Focal Onset Alzheimer's Disease
What is Alzheimer’s Disease? (Definition/Background Information)
- Alzheimer’s Disease (AD) is a common, progressive brain disorder that impacts one’s memory, language, and thinking ability. It is the most common type of dementia, and is typically seen in individuals older than 60
- Individuals with Alzheimer’s Disease experience a slow loss of brain function, affecting their ability to remember and think with clarity (memory loss)
- Due to the progressive nature of the disease, symptoms worsen over time, making it difficult for individuals with the condition to live on their own, and to take part in day-to-day routine/regular activities
- No cure has been developed for Alzheimer’s Disease, though treatments are available to help treat certain symptoms
Alzheimer’s Disease may be classified into the following subtypes based on clinical presentation, inheritance pattern, and brain imaging studies:
- Typical Alzheimer Disease: Typical Alzheimer's disease is the most common form, characterized by progressive cognitive decline, memory loss, and changes in behavior. It often follows a predictable pattern of cognitive decline associated with specific pathological changes in the brain, such as the accumulation of beta-amyloid plaques and tau protein tangles
- Familial Alzheimer Disease: Familial Alzheimer's disease is a rare genetic form of the condition that is passed down through families. It typically has an earlier onset and is caused by mutations in specific genes, such as APP, PSEN1, and PSEN2
- Early-Onset Alzheimer Disease: Early-onset Alzheimer's disease refers to cases that begin before the age of 65. It may be sporadic or familial and tends to progress more rapidly than late-onset forms
- Late-Onset Alzheimer Disease: Late-onset Alzheimer's disease is the most common form and typically occurs after the age of 65. It is often sporadic and progresses more slowly
- Limbic-Predominant Alzheimer Disease: This subtype primarily affects the limbic system of the brain, leading to specific cognitive and behavioral changes. It often presents with memory problems and mood disturbances
- Hippocampal-Sparing Alzheimer Disease: In this subtype, the hippocampus, a brain region crucial for memory, is relatively spared, while other areas of the brain are more affected. This leads to distinct clinical features
- Minimal Atrophy Alzheimer Disease: Minimal atrophy Alzheimer's disease is characterized by cognitive decline without significant visible brain atrophy on imaging studies. It suggests that the cognitive symptoms may be primarily driven by molecular changes rather than structural brain changes
Who gets Alzheimer’s Disease? (Age and Sex Distribution)
- Alzheimer’s Disease occurs past the age of 65 years. This happens frequently and is known as Late Onset Alzheimer’s Disease
- It is infrequent below this age range. When it occurs below this age group, it is termed Early Onset Alzheimer’s Disease
- Generally, females are slightly more prone to this disorder than males
- No particular race or ethnic preference has been observed, and this disorder is observed worldwide
What are the Risk Factors for Alzheimer’s Disease? (Predisposing Factors)
There are a host of factors that could potentially increase the risk for Alzheimer’s Disease (AD). Some may be controlled, while others are unchangeable and may be relentless. These include:
- Advancing age: The older the individual is over 65, the higher is the risk. This is the single most important predisposing factor for AD
- Genetic causes: Individuals having a family history of Alzheimer’s disease, particularly those having a close relative or a sibling
- Direct risk factors for Alzheimer’s include high blood pressure, uncontrolled diabetes (type 2), high blood levels of the amino acid homocysteine (a condition termed as homocystinuria), depression, and past head injury (which maybe prolonged)
- Individuals with mild cognitive impairment, mild loss of memory and impairment of language, thinking skills, due to old age
- Food and lifestyle habits, such as smoking of tobacco, cholesterol (high levels of LDL), atherosclerosis due to fat build-up, eating less fruits and vegetables, seclusion from social life, and aloofness, and leading a sedentary life
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases one’s chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Alzheimer’s Disease? (Etiology)
Alzheimer’s Disease (AD) is believed to be aided by a combination of factors.
- Genetic mutations are thought to be a major factor in determining who will be affected by Alzheimer’s Disease. Research has found that mutations on the Apolipoprotein E (apoE) gene are common in people with the condition, leading to the belief that it could be a causative factor
- Lifestyle factors are also thought to play an important role in determining who might be affected by AD. Individuals with high blood pressure, diabetes, and heart problems, may be more likely to develop this brain disorder
- Alzheimer’s Disease may also be caused by trauma and injury to the brain
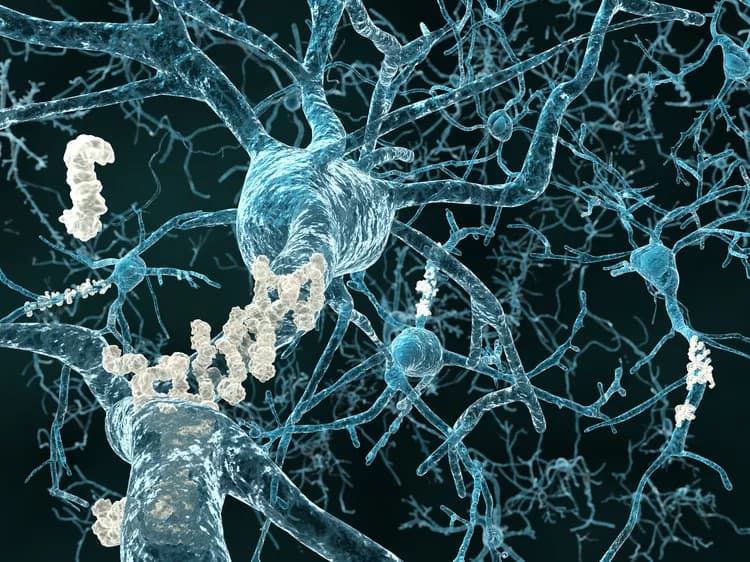
According to research scientists, Alzheimer’s Disease develops slowly due to atrophy of the brain, when brain cells (neurons) begin to die for unknown reasons. It is suspected that certain abnormal structures, called amyloid plaques and tangles, may be responsible for nerve cell injury and death.
What are the Signs and Symptoms of Alzheimer’s Disease?
Common signs and symptoms of Alzheimer’s Disease include:
- Memory loss/problems - these are early indicators and may include (for example) trouble recollecting recently learned information, misplacing items of regular use, getting lost in known places, forgetting familiar faces, or forgetting to pay for services at shops or restaurants
- Difficulty performing daily activities, difficulty reading, or sleeping
- Agitation
- Depression
- Anxiety
- Mood swings
- Poor judgement
- Mental retardation
- Impaired social behavior
The signs and symptoms of individuals may vary from one to another and can be mild or severe.
How is Alzheimer’s Disease Diagnosed?
An early recognition of the signs and symptoms followed by an accurate diagnosis of Alzheimer’s Disease can aid in providing prompt medical attention and care to the affected individuals. A variety of tests may be conducted to diagnose Alzheimer’s Disease, which include:
- Physical exam with a comprehensive evaluation of medical history, including collecting details on any underlying conditions/disorders and their progression
- Neurological examination
- CT, MRI, and PET scans to view the brain and determine if any medical issues are present
- Blood tests may be used to check for thyroid disorders
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of Alzheimer’s Disease?
- Alzheimer’s Disease (AD) is the most common cause factor for dementia (between 60-80% of dementia cases develop due to AD). Dementia is a type of disorder accompanied by a collection of symptoms that indicate brain impairment and loss of brain function
- Since AD is a progressive disorder, it can create difficulties in the life of the individual, and their family members (both functional and cognitive decline is noted)
- As symptoms worsen, it becomes more and more difficult for those affected by the condition to carry out even simple, everyday tasks. They are usually unable to live on their own
- Severely impaired brain function during the advanced stages of Alzheimer’s Disease
The symptoms may also worsen resulting in an early death. Some individuals may live for about 20 years following a diagnosis of Alzheimer’s Disease, although the average lifespan is between 4-8 years.
How is Alzheimer’s Disease Treated?
- Currently, there exists no cure for Alzheimer’s Disease. The quality of life of the affected individuals can be improved through appropriate medical management of the condition
- There are various treatment measures to help treat the symptoms of the disease. These include:
- Delaying progression of the condition through medications
- Use of medications to treat behavioral issues and to aid the individual in helping him/her performing their daily activities
- Use of therapy sessions (helps an individual to better remember basic activities, things, etc.)
Enlisting the support of family members and friends is important in the care of the patient.
How can Alzheimer’s Disease be Prevented?
- Due to the fact that Alzheimer’s Disease is likely caused by multiple factors, it is difficult to prevent the disease
- However, preventative measures may be taken to lower the likelihood of developing the disorder. These may include adopting a healthier lifestyle such as through:
- Mental stimulation/brain exercises through simple brain games, learning activities (such as a musical instrument or a language), etc.
- Regular exercising
- Having a healthy and balanced diet
- Proper management of high blood pressure and diabetes
What is the Prognosis of Alzheimer’s Disease? (Outcomes/Resolutions)
- As the length of time with Alzheimer’s Disease increases, symptoms of the disease progressively worsen. In most cases, individuals lose their ability to function in day-to-day life making them dependent upon their family members, or else by having to move into a facility of care (such as a nursing home)
- Normally, a life-long management of the condition is necessary. Early detection and aggressive management of Alzheimer’s dementia with regular health checkups and supportive care are essential. This can help prevent further (rapid) deterioration of the condition and help sustain the quality of life
- Generally, with Alzheimer’s Disease, an individual may live anywhere between 3-20 years, after onset of the condition. Alzheimer’s that develop early and rapidly, and progress at a faster pace, bring about the worst outcomes. Death may result from infections, such as pneumonia, or failure of vital organs
Additional and Relevant Useful Information for Alzheimer’s Disease:
There are voluntary organizations and support groups for Alzheimer’s Disease that provides counsel, help, and understanding, to the affected individuals and families.

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.