What are the other Names for this Condition? (Also known as/Synonyms)
- Endometriosis of other Specified Sites
- Endometriosis, Site Unspecified
- Uterus Corpus Adenomyosis
What is Endometriosis? (Definition/Background Information)
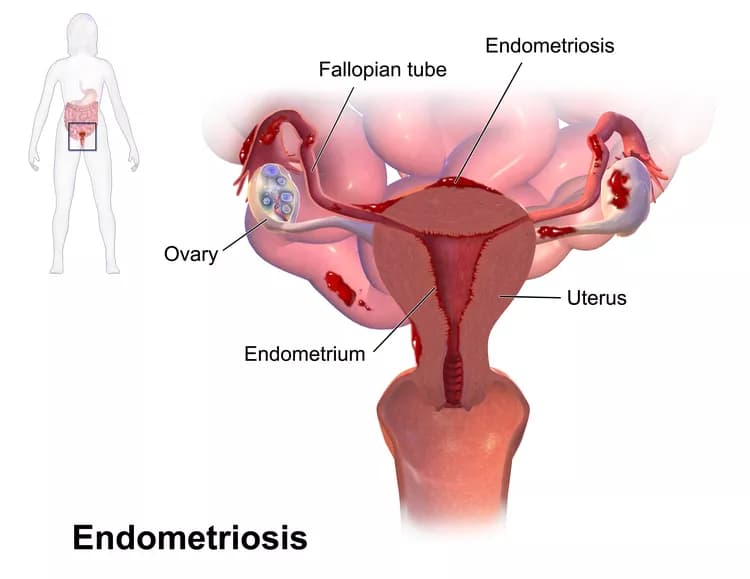
- The endometrium is the lining of the uterus that proliferates during the menstrual cycle and sheds during menstruation. This cyclical pattern is created by the response of glands and blood vessels present in the endometrium to fluctuating levels of estrogen and progesterone during the menstrual cycle
- Endometriosis is the presence of benign endometrial tissue (endometrial stroma and glands) in abnormal locations outside of the uterus in the pelvis and occasionally, the abdomen and elsewhere. It is a common condition that may be either asymptomatic or cause pelvic pain (most common symptom), irregular bleeding, and infertility
- Ovarian cysts comprising of endometrial tissue are commonly observed. Endometrial lesions are also sometimes located on the bowel, rectum, bladder, ureters and the lining of the pelvis (peritoneum)
- Endometrial tissue outside of the uterus responds to cyclic hormone changes just as normal endometrial tissue does by bleeding. The blood typically cannot exit the body and eventually forms scar-like lesions on pelvic structures
- A diagnosis of Endometriosis is often difficult and challenging. Biopsy of the endometrial tissue following a laparoscopy is the only definitive method to diagnose the condition. It is noted that in some women, a diagnosis of Endometriosis may be delayed by several years
- Though there is no cure for the condition, it can be managed through medications, oral contraceptives, and the use of hormone derivatives. The prognosis is generally good, though pain and discomfort may last for years, or even up to menopause
Who gets Endometriosis? (Age and Sex Distribution)
- According to studies, Endometriosis affects up to 22% of menstruating women; although many cases remain asymptomatic. Most women are in the age range of 25-35 years, at the time of diagnosis
- Around 20-50% of women with infertility are affected
- Around 40-50% of women with pelvic pain are affected
- The condition is observed worldwide and all racial and ethnic groups are generally at risk
What are the Risk Factors for Endometriosis? (Predisposing Factors)
The risk factors of Endometriosis may include the following:
- Positive family history: First degree relatives of women with Endometriosis are at a greater risk for developing the condition
- Anatomic malformations blocking the reproductive outflow tract
- First menstrual cycle at an early age
- Frequent menstrual cycles or periods lasting greater than 7 days
- No prior pregnancy
- Exposure to diethylstilbestrol in utero (mother receiving the drug when pregnant)
- Exposure to dioxin and dioxin-like compounds found in industrial waste
- Low birth weight (of the woman)
It is important to note that having a risk factor does not mean that one will get the condition. A risk factor increases one's chances of getting a condition compared to an individual without the risk factors. Some risk factors are more important than others.
Also, not having a risk factor does not mean that an individual will not get the condition. It is always important to discuss the effect of risk factors with your healthcare provider.
What are the Causes of Endometriosis? (Etiology)
Many theories exist that offer an explanation of how Endometriosis might develop, although the exact cause of extrauterine endometrial lesions is unknown. It is thought that a combination of factors may be responsible for the development of Endometriosis.
- Retrograde menstruation from the uterus through the fallopian tubes and into the peritoneum (opposite direction of normal flow) is one potential mechanism by which endometrial tissue could seed extrauterine locations
- Another theory involves the spread of endometrial cells through blood vessels or lymphatics to other pelvic structures
- Metaplasia: It is said that during uterus formation (embryogenesis) or later in adulthood, some “normal tissues” undergo abnormal changes resulting in the presence of endometrial tissue outside the uterus
- Hormonal influences could also potentially induce the transformation of undifferentiated cells in pelvic organs into endometrial cells. Inhibition of estrogen activity on extrauterine endometrial tissue is one goal of treatment. Based on medical research, it is believed by many that estrogen production by the body makes the condition worse
- Other factors that are thought to play a role include genetic factors (the condition may run in the family), immune system dysfunction, and environmental factors
What are the Signs and Symptoms of Endometriosis?
Most patients of Endometriosis are asymptomatic. The signs and symptoms depend on the location of the endometrial lesions and may generally include:
- Chronic or cyclic pelvic pain - it is the most commonly noted presentation
- Pain early in the menstrual cycle; pain after menstruation
- Discomfort or pain during bowel movements and urination
- Pain while/after having sex
- Irregular and/or excessive bleeding
- Backache (in the lower back)
- During menstruation, some women may have constipation/diarrhea and abdominal bloating
- Tiredness
The location of the endometrial tissues may vary from one woman to another. In the pelvis, involving the reproductive system, it may be found at the following sites:
- Fallopian tube
- Ovary
- Vagina
- Septal wall between the vagina and rectum (rectal-vaginal septum)
- Pouch of Douglas (rectouterine pouch)
- Cul-de-sac (between the uterus and rectum)
- Uterosacral ligament
- Urinary bladder and ureter
- Peritoneum
Other sites for the endometriosis lesions may rarely include:
- Small and large intestine, including appendix and rectum
- Surgical scar sites such as from a C-section or laparoscopy
- Central nervous system (brain and spinal cord)
- Lung
- Skin
How is Endometriosis Diagnosed?
In many cases, a diagnosis of Endometriosis may be delayed due to an absence of significant signs and symptoms, or since the pain associated with Endometriosis is noted around menstruation. The diagnosis may be undertaken using the following tools:
- Physical examination with detailed medical history: A pelvic (gynecological) examination and palpation of pelvic organs can suggest a diagnosis of Endometriosis. In such cases, the treatment may be started without any additional tests being performed
- Laboratory tests, such as complete blood count (CBC), cancer antigen 125 (CA 125), urinalysis, and vaginal swab cultures, may be undertaken to rule out pelvic pain, due to a sexually-transmitted infection
- Radiological imaging studies of the pelvic region, including ultrasound and MRI scans
- Transvaginal ultrasound may aid in investigation of pelvic pain
- Examination of an endometrial biopsy sample obtained during laparoscopy or laparotomy is necessary to confirm the diagnosis. Examination of the biopsy under a microscope by a pathologist is considered to be the gold standard, in arriving at a conclusive diagnosis. It is observed that in some cases, the healthcare professionals must have a high index of suspicion of the condition to diagnose the same
- Suspected Endometriosis may be treated without confirming with endometrial biopsy, if other causes of pelvic pain are ruled out
- However, the symptoms of Endometriosis may be similar to those in other conditions, such as pelvic inflammatory disease. Hence, other causes of pelvic pain and infertility must be ruled out
Many clinical conditions may have similar signs and symptoms. Your healthcare provider may perform additional tests to rule out other clinical conditions to arrive at a definitive diagnosis.
What are the possible Complications of Endometriosis?
The following complications of Endometriosis may be expected:
- Pelvic pain may be severe and debilitating
- Formation of scar tissue and adhesions (abnormal formation of fibrous bands between neighboring tissues and/or organs); severe cases of adhesions may infrequently lead to a condition termed “frozen pelvis”, where organs may fuse together
- Infertility is associated with Endometriosis in 20-40% of cases. However, it is not completely understood how Endometriosis is responsible for infertility. However, approximately 60% of women with mild Endometriosis are still able to conceive within one year, even without treatment
- Complications may occur in the early or late stages of pregnancy, and can include ectopic pregnancy, pre-eclampsia, and preterm births
- Pelvic cysts may rupture causing pain, with risk of infection
- Endometriosis is associated with a higher risk of ovarian cancer; though, it is not a pre-malignant condition
- Overall quality of life may be affected
How is Endometriosis Treated?
The treatment of Endometriosis is based on the severity of symptoms and the location of endometrial lesions. In many cases, long-term treatment may be necessitated. Also, presently, it is reported that there is no complete cure for Endometriosis.
- Pain relievers, such as NSAIDs (e.g., acetaminophen, ibuprofen, or naproxen) may provide relief of mild symptoms
- Oral contraceptives may also provide pain relief by interrupting the menstrual cycle
- Hormonal therapy: Hormone derivatives including progestins, testosterone and gonadotropin releasing hormone (GnRH) may be prescribed; these work by antagonizing the effects of estrogen or suppressing the cyclic hormone cycle
- Surgery to remove the endometrial lesions may improve infertility and pain, but the lesions may recur. Laparoscopic procedures may be recommended for women with mild cases of Endometriosis
- Pain that is unresponsive to medication may improve following a hysterectomy (removal of the uterus)
Women who find it difficult to conceive may be advised to take the help of assisted reproductive technologies.
How can Endometriosis be Prevented?
Currently, there are no known preventative measures for the development of Endometriosis. However, the following may be considered to reduce impact of the condition:
- Availing early treatment
- Patient education about the condition
- Providing counseling and support
The use of oral contraceptives (birth-control pills) or bringing about lifestyles changes (via food and exercise) are not presently known to aid in preventing Endometriosis.
What is the Prognosis of Endometriosis? (Outcomes/Resolutions)
There is no cure for Endometriosis, but the symptoms can usually be managed through adequate treatment.
- In 25% of the women, the symptoms resolve with or without treatment in less than one year
- Many women will have symptoms until menopause, although medication and surgery can improve pain and infertility
- Surgery can also improve the chances of women becoming pregnant
- Symptoms may recur in patients who undergo surgery to remove endometrial lesions
- A hysterectomy with removal of the ovaries and fallopian tubes is most effective for a complete resolution of the condition in many women
Additional and Relevant Useful Information for Endometriosis:
- There is no evidence of any association between Endometriosis and miscarriages
- Vaginal hysterectomy is a surgical procedure characterized by the surgical removal of the uterus through an incision within the vagina
The following article link will help you understand vaginal hysterectomy:
https://www.dovemed.com/common-procedures/procedures-surgical/vaginal-hysterectomy/

Related Articles
Test Your Knowledge
Asked by users
Related Centers
Related Specialties
Related Physicians
Related Procedures
Related Resources
Join DoveHubs
and connect with fellow professionals
0 Comments
Please log in to post a comment.